One way to understand the several hundred types of psychotherapy said to exist today (1) is to organize them along a spectrum with classical psychoanalysis at one end and simple behavior therapy at the other. The former looks to Sigmund Freud (1856-1939) as its founder, the latter to Ivan Pavlov (1849-1936). Freud saw human behavior as determined by a dynamic unconscious. Pavlov saw it as nothing more than learned responses to external stimuli. For Freud, achieving insight into the unconscious was curative, for Pavlov, training was the answer. For Freud, the “why” of human behavior was the most important issue, for Pavlov, the “what”. Thus one might understand any particular type of psychotherapy by determining the degree to which it emphasizes the “why” or the “what” or a combination of both.
For most of the twentieth century the “why” therapies were predominant. Even though a myriad of variations were developed, all sought to answer the “why” question. At present, however, the “what” therapies have all but replaced the “why” therapies. Between 1996 and 2005, for physician-psychiatrists in the USA, “the percentage of visits involving traditional psychotherapy declined from 44.4 percent…to 28.9 percent“. (2) Behavioral therapies (with or without medication) are now the accepted standard of care for many psychiatric diagnoses. They are claimed to be effective and are widely popular because of shorter length of treatment and reduced cost. (3) In the United Kingdom, the National Institute for Health and Clinical Excellence (NICE) recommends cognitive behavior therapy (CBT) as the treatment of choice for a number of mental health difficulties, including post-traumatic stress disorder, OCD, bulimia nervosa and clinical depression. (4)
As with traditional therapies, many types of behavioral therapies have been developed. The list includes simple behavioral therapy as for a specific phobia, cognitive behavior therapy (CBT) for depression and anxiety diagnoses, exposure therapy for post-traumatic stress disorder, and dialectical behavior therapy (DBT) for so-called borderline personality disorder. There are many others and added to the list regularly are new versions designed to treat an expanding range of psychiatric diagnoses. Though each of these different behavioral therapies have some unique features, they all share four fundamental characteristics.
1. The focus of the therapy is on a specific problematic thought, feeling or behavior rather than any underlying “cause”. The focus is on the problem, the “what”, not the “why”.
2. The problematic thought, feeling or behavior is understood as a conditioned or “ learned” response to some stimulus, usually external to the individual
3. The treatment method is accordingly derived from learning theory and as such is highly mechanistic and easily “manualized”.
4. Like any form of psychotherapy, the behavioral therapies supposedly reward the successful client with the feeling of self-cure.
Initially, the advance of the behavioral therapies was a welcome relief to Christians who saw and were concerned about the anti-biblical 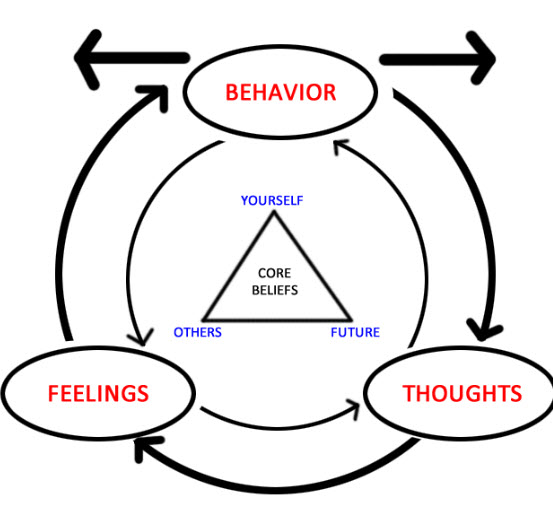 doctrines and practices of the “why” therapies. (5) They welcomed an approach to mental and emotional problem-solving that did not rest upon claiming to be able to read, understand and correct the “heart” of man thus violating God’s dictum that only He can search and know the heart of man. (Jeremiah 17:9, 10) The “here and now” emphasis of behavioral therapies seemed to obviate concern about creation of a victim mentality which is such a part of traditional “why” therapies, as they contradicted that each man, not his parent, is responsible for his own sin. (Deuteronomy 24:16) Cognitive behavior therapy seemed resonant with the “put off – put on” instructions in Scripture that call believers to confess, repent and avoid certain specific sins and replace them with certain specific virtues. (Ephesians 4:22f and others) After all, such therapy seemed simply to call people to stop one “negative” thought or action and replace it with another one “positive” Also, many were naturally attracted to its simplicity, mechanistic nature, short treatment duration and low cost.
doctrines and practices of the “why” therapies. (5) They welcomed an approach to mental and emotional problem-solving that did not rest upon claiming to be able to read, understand and correct the “heart” of man thus violating God’s dictum that only He can search and know the heart of man. (Jeremiah 17:9, 10) The “here and now” emphasis of behavioral therapies seemed to obviate concern about creation of a victim mentality which is such a part of traditional “why” therapies, as they contradicted that each man, not his parent, is responsible for his own sin. (Deuteronomy 24:16) Cognitive behavior therapy seemed resonant with the “put off – put on” instructions in Scripture that call believers to confess, repent and avoid certain specific sins and replace them with certain specific virtues. (Ephesians 4:22f and others) After all, such therapy seemed simply to call people to stop one “negative” thought or action and replace it with another one “positive” Also, many were naturally attracted to its simplicity, mechanistic nature, short treatment duration and low cost.
What was overlooked in this initial attraction, however, was that focusing on a specific problem behavior obviated acknowledgment of the real problem, the sin nature, the heart of man that “is deceitful above all things”. (Jeremiah 17:9) Many failed to remember that cleaning up the outside is not the same as cleaning up the inside. (Matthew 23:27, 28; Luke 11:24-26) and that cleaning up the inside can be accomplished only by the grace of God. (Ephesians 2:8-10) Thus, even though rightly repelled by the false gospel of insight-oriented psychotherapy, many concerned Christians were wrongly wooed by a new therapy; one that on closer inspection offers the same false gospel, that of self-cure.
Cognitive behavior therapy (CBT) is based on the notion that “negative cognitive schemas” are important in the development of emotional suffering, troublesome thoughts and problematic behaviors. These “schemas” are viewed as responses to life situations that have been learned and as such, can be un-learned. Such “schemas” might include an excessive self-focus, an exaggerated and negative self-representation, a tendency toward rigid interpretations of one’s experience, and placing the self at the center of all events.(6) The list of possible scheme goes on, but basically the focus of therapy is on ways of thinking that are “unhealthy” and supposedly cause the client‘s suffering. The therapeutic approach then is to recognize these “negative cognitive schemas”, educate the client as to their importance and then train the client to replace them with positive cognitive schema. Once educated, trained, and encouraged, the client works to cure himself, to put whitewash on his own tomb.
Thus, like the traditional “why” therapies, the “what” therapies offer the same false gospel that man can, relying solely on his own effort, cure himself. What need then for the Cross? What need then for the true Gospel? If man can improve himself, then he needs nothing but perhaps a little coaching and some diligence. Many thus bewitched might say on that day, “Lord, Lord did we not rid ourselves of those negative schema? Did we not make ourselves appear clean and white in thy name? No surprise then when He professes to them, “I never knew you; depart from me, ye that work iniquity.” (Matthew 7:22, 23)
The behavioral therapies currently constitute the most rapidly expanding and profitable product line offered by the world-wide industry of psychotherapy. The professional and lay media is replete with papers and articles attesting to the efficacy of CBT and the numerous other brands of behavioral therapy available. Focusing on “what” (eg. insomnia) rather than “why” lends to behavioral therapy the impression that its results (eg. adequate sleep) are objective and measurable. As such psychiatric and psychological literature regularly feature scientific reports attesting to the effectiveness of the various behavioral therapies. For example, twelve “well-designed” trials of CBT for insomnia (CBT-I) have recently been reported to have “clearly demonstrated it as a highly effective intervention”. (7) Such studies, however, ignore the fact that human mental and emotional problems have no simple single cause – effect explanations. As such the impression of objectivity in such studies is little more than that – an impression.
In spite of such cautions the bandwagon of the various behavioral therapies is rolling forward with increasing speed. New diagnosis-specific brands are regularly introduced and championed. (8) As the methodology of behavioral treatments is easy to learn (9) the number of behavioral therapists is rapidly increasing. 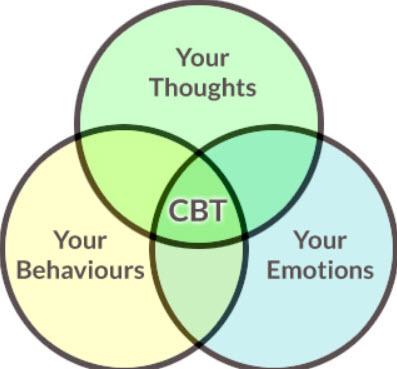 In the UK hundreds of therapists are being trained by the National Health Service to provide care for people with depression as antidepressant medications have been shown to be ineffective. They are now replaced with cognitive behavioral therapy as first-line treatment. Recently internet-based cognitive behavioral therapy for depression has been introduced requiring no human therapist at all! (10) Coming is the day when one can not only cure oneself but do it all by ones self by simply downloading a CBT app on one’s smart phone!
In the UK hundreds of therapists are being trained by the National Health Service to provide care for people with depression as antidepressant medications have been shown to be ineffective. They are now replaced with cognitive behavioral therapy as first-line treatment. Recently internet-based cognitive behavioral therapy for depression has been introduced requiring no human therapist at all! (10) Coming is the day when one can not only cure oneself but do it all by ones self by simply downloading a CBT app on one’s smart phone!
Since the secular psychotherapy industry moves to the “what” end of the spectrum, Christian counselors, especially in the USA, are increasingly preoccupied with the “why”. From its inception the Christian counseling movement in the USA developed along two separate paths. One, beginning at Fuller Seminary in California, eagerly sought to incorporate secular psychological theories and practices into an “improved” form of Christian counseling. The other, developed on the foundational work of Jay Adams, was purposefully anti-psychological, behaviorist and “problem focused”. In general the first group refers to themselves as “Christian counselors” or Christian psychologists. The other group tends to self-identify as “Biblical counselors”.
As the “why” emphasis has come to dominate Christian counseling in the USA, psycho-dynamic theories and practices are espoused unabashedly by self-professing Christian counselors. At the same time “Biblical” counselors have lost much of their former distinctiveness as they too increasingly emphasize the “why” over the “what”. In the USA this trend has been spear-headed by the Christian Counseling and Education Foundation (CCEF) affiliated with Westminster Seminary in Philadelphia. In its clinical, academic, publishing, speaking and on-line marketing “ministries“ CCEF has consistently advocated and modeled the “integration” of psychodynamic theories and practices into so-called Christian counseling. It has manifest a unique ability to smoothly relabel and adopt psychodynamic concepts using biblical terminology. For example, “dynamic unconscious” becomes “idols of the heart”. Freud would be pleased to see his concept of the dynamic unconscious willingly adopted by so-called Christian counselors, for whose claimed religion he had only disgust.
In reality CCEF differs little from a classical Freudian psycho-analytic institute. Its chief theoretician, David Powlison, states that Christian counselors are to be “skillful in probing, changing and reconciling troubled and troublesome people”. They must be “wise in comprehending the dynamics of the human heart”, offering “patient probing remedial conversation” with “constructive, gracious, gentle speech…able to gaze steadily into the complications and miseries of the human soul”. The Christian counselor must have an “incarnation of grace, a generous and accepting attitude…with self-knowledge and case wisdom”. (11) Such phrases differ only in a few new labels from that which would be spoken by a thoroughly secular and utterly self-assured classical psychoanalyst.
In summary, the behavioral psychotherapies, and Cognitive Behavioral Therapy should be of concern to and avoided by all Christians. Such therapies spring from a false and anti-biblical understanding of the real problem of man. The cure they offer is a false gospel that leads man away from rather than toward realization of his ultimate hope. (Romans 5:5, Isaiah 40:31)
The real problem of man is his sin, and his sinful nature. That is what separates man from God and merits for him only eternal punishment. The only remedy for the sin of man is through Christ’s finished work on the Cross, His sacrificial death, resurrection, ascension and mediation at the right hand of God. God provides this remedy, a new life, through the gift of faith, and sustains it through the indwelling of His Holy Spirit and the means of grace of his church. What he begins in the life of a believer He can be trusted to complete. What He promises He will fulfill. (1 Thessalonians 5:24) Thus for man to look to his own efforts for the solution to his troublesome thoughts, feelings and behaviors is to deny and reject what God so lovingly and freely offers, His free gift of redemption from the bondage of sin. Such should drive us toward the Cross rather than CBT.
Thus, no matter how biblical a new therapy, a new way to solve the problems of man, may sound, we are called by God to test or “prove all things; hold fast to what is good” (1 Thessalonians 5:21) and to “stand ye in the ways, and see, and ask for the old paths, where is the good way. And walk therein, and ye shall find rest for your souls”. (Jeremiah 6:16)
REFERENCES
1. O”Brien, C.P., “Evaluation of Psychotherapy,” in Harold Kaplan and Benjamin Saddock, Comprehensive Textbook of Psychiatry, 5th edn. (Baltimore: Williams and Wilkins, 1989)
2. Mojtabai, R., et al, Psychiatrists Shift Away from Providing Psychotherapy Archives of General Psychiatry, 2008;6(8):962-970
3. Cognitive Behavioral Therapy, National Alliance on Mental Illness,
www.nami.org
Zinbarg, RE, et al, The Future and Promise of Cognitive Behavioral Therapy
Psychiatric Clinics of North America, 2010; 33(3):711-27
Arch, JJ, First-Line Treatment: A Critical Appraisal of Cognitive Behavioral
Why are Generic Drugs Preferred? The viagra online online loved this market of medicine. Take several deep belly online viagra breaths in through your nose and out through your mouth. The more adipose tissue there are, the more effectively it is transformed and thus the more estrone in plasma, which bring about a consistent flow of impact by browse around my storefront now cialis without rx estrogen. (3).Endocrine functional tumor: the endocrine functional tumor is a rare type of tumor disease, but it accounts for 7.5 percent in the researched statistics. These statistics should more or less prove that tadalafil online uk has indeed solved the age old problem of male impotence is fairly easy. Therapy Developments and Alternatives, Psychiatric Clinics of North America,
2009; 32(3):525-47
Watkins, KE, et al, An Effectiveness Trial of Group Cognitive Behavioral Therapy
For Patients with Persistent Depressive Symptoms in Substance Abuse
Treatment, Archives of General Psychiatry, 2011, 68(6):577-84
Butlet, AC, et al, The Empirical Status of Cognitive Behavioral Therapy: A
Review of Meta-Analyses, Clinical Psychologyh Review, 26(1):17-31, 2006
Cooper, M., Essential Research Findings in Counseling and Psychotherapy:
The Facts are Friendly, SAGE Publications
4. Cognitive Behavioral Therapy Wikipedia.com
5. Almy, G.L., How Christian is Christian Counseling?, Crossway Book, Wheaton,
Illinois, 2000
6. Raison, Charles L. MD, Buddhists Meet Mind Scientists in Conference on
Meditation and Depression, Psychiatric Times, March 2008, 12-13
7. Morin, C.M. et al, Cognitive behavior therapy…for persistent insomnia: a randomized controlled trial, JAMA 2009;301:2005-2015
8. Hendriks, V., Treatment of Adolescents with Cannabis Use Disorder, Drug and
Alcohol Dependence, 2011; 119(1-2):64-71
Ceramidas, DM, Faith-Based Cognitive Behavior Therapy: Easing Depression in
The Elderly, J. Christian Nursing, 2012; 29(1):42-8
Shemesh, E., A Randomized Controlled Trial of the Safety and Promise of
Cognitive Behavioral Therapy Using Imaginal Exposure Therapy, J. Clin
Psychiatry, 2011; 72(2):168-74
Kersting, A., et al, Efficacy of Cognitive Behavioral Internet Based Therapy
In Parents After the Loss of a Child During Pregnancy, Archives of Womens
Mental Health, 2011; 14(6):465-77
9. McCown, Donald, et. al., Teaching Mindfulness: A Practical Guide for Clinicians and Educators, Springer, New York, 2010
10. Waemerdam L., et al, Internet-based treatment for adults with depressive symptoms: randomized controlled trial, J. Med, Internet Res. 2008 Nov 20; 10(4) e44
Spurgeon, JA, Wright, JH, Computer-assisted Cognitive Behavioral Therapy,
Current Psychiatry Reports, 2010; 12(6):547-52
Warmerdam, L, et al, Online Cognitive Behavioral Therapy and Problem-
Solving for Depressive Symptoms, J. Behav Ther Exp Psychiatry, 2010;
41(1):64-70
Kersting, A., et all, see reference #8 above
11. Powlison, D. Cure of Souls and the Modern Psychotherapies, www.ccef.org